
If you have been following my blog, you know that for 2019 I have decided to study twelve different characteristics of resilience, one for each month.
The characteristic I am studying in JANUARY is JUMPING INTO ACTION. In the wider context, this means dealing with the stress that comes into my life in an active rather than a passive way. Last week, I shared some basic action steps suggested by the American Heart Association.
But I couldn’t let the month go by without talking action in the physical sense: pounding the pavement in a daily walk or run, slugging it out with a punching bag, or throwing down some push-ups or squats.
I am talking about exercise.
This is literally JUMPING INTO ACTION.
Nike sums it up nicely with their trademark phrase: JUST DO IT.
I have a long-standing interest in the mental benefits of exercise. In fact, it was the first topic I studied and published on back in grad school.
To bring you the most up-to-date information in this post, I turned to a book that I got last year for Christmas: The Exercise Effect on Mental Health: Neurobiological Mechanisms edited by German researchers Henning Budde and Mirko Wegner.1
(Yes, I ask for neuroscience books for Christmas. I am that much of a nerd.)
This book summarizes the main findings regarding exercise’s ability to improve cognitive function and treat (maybe even prevent) mental illness.
For this post, I will answer the following questions:
- How are depression and illness related?
- What evidence do we have that physical activity can actually prevent a downward slide into depression or anxiety?
- If a person already suffers from depression or anxiety, what evidence do we have that exercise is an effective treatment?
- Assuming that exercise is helpful, what kinds of exercise (mode, frequency, duration) are best?
How are depression and illness related?
Researchers say that depression and illness have a “bi-directional” relationship, meaning that illness can lead to depression, but depression can also lead to illness:

Both directions are likely true.
Evidence that depression leads to physical problems came from a survey conducted by the World Health Organization of 47,000 citizens from 17 countries.2 This survey showed that suffering from depression increased the odds of subsequently suffering from ten chronic health conditions spanning cardiovascular, respiratory, gastrointestinal, metabolic, and chronic inflammation / pain disorders.
Depression likely impacts our health both directly and indirectly.
Directly, we know that depression triggers biological cascades like inflammation that later contribute to physical and mental distress.
Indirectly, depression promotes negative behaviors like drinking, taking drugs, physical inactivity, and careless diet.
Conclusion: Depression and illness are inter-related: illness can lead to depression, but depression can also lead to illness.
Can Exercise Prevent Depression and Anxiety?
The medical journal Lancet recently reported that in a population sample of 1.2 million Americans, those who exercised more – but otherwise matched non-exercisers in terms of sociodemographics and physical characteristics like Body Mass Index – experienced over 40% fewer days of poor mental health in a month.3
This is a compelling finding, but it does not really prove a cause and effect relationship between exercise and better mental health.
It’s more like taking a snapshot of all of these people at one point in time. In this snapshot, it is just as likely that depression caused the inactivity as it is that the inactivity led to depression.
And exercise and fewer days of poor mental health could both be caused by a third factor, like higher self-esteem and more motivation.
To sort out cause and effect, researchers have to do more than take a simple snapshot. They have to follow individuals in a population over time, like following their story on Instagram.
At the beginning of the story, the researchers identify the participants’ lifestyle habits, like exercise, nutrition, etc. Then they track what happens to them later in terms of mental health.
The vast majority of these “story”-type studies show that participation in physical activity decreases the risk of poor mental health later.4
Even a little bit helps. Researchers in Sweden reported that just 120 minutes of leisure activities like gardening or walking – less than 25 minutes a day in five-day workweek – cut the risk of depression by over 60% compared to those who stayed sedentary.5
Conclusion: The majority of scientific evidence suggests that exercise can prevent mental health problems.
Is Exercise an Effective Treatment for Depression and Anxiety?
The two main lines of treatment for depression and anxiety are drugs and counseling, the most popular being cognitive behavioral therapy.
Here’s an interesting side note: When patients themselves are surveyed about their preference between the two, about three-quarters of them prefer counseling.6 In spite of this, the use of psychotherapy has declined in the United States while the use of antidepressant drugs has increased.7
Is exercise an effective alternative?
Many clinical trials have tried to answer this question.
The Cochrane Group, a network of almost 40,000 researchers and healthcare professionals, has combined clinical data from dozens of independent studies into a much larger, “meta” dataset.
Results from these “meta” studies have shown that exercise is just as effective as antidepressant drugs in reducing symptoms of depression.8
Other research groups have found similar results for treatment of anxiety.9
Conclusion: The majority of scientific evidence suggests that exercise can be just as effective as other standard therapies in treating depression and anxiety.
Science nerds like me are not just interested in whether or not exercise protects mental health. We also want to understand how this happens. Several plausible explanations have been put forward:10
- Some of the benefit may be purely mental – increased physical fitness gives one a sense of accomplishment and higher self-esteem.
- Exercise may also provide a needed distraction (sort of a mini vacation) from the stresses of life.
- Some of the benefit may also be emotional. Group exercise provides social support and encouragement.
- Finally, some
of the benefit may be neurobiological.
- Exercise increases the levels of natural opioids called beta endorphins.11 This is what is thought to cause the “runner’s high.”
- Exercise re-trains hormonal systems12 so that less stress hormones get released in potentially stressful situations.
- Exercise decreases levels of inflammatory chemicals known to produce depressive symptoms.13
- Exercise increases metabolism and improves blood flow in brain areas affected by depression.14
- Exercise increase production of growth factors that help brain cells grow, survive, and thrive.15 Again, researchers have noticed that an increase in growth factors specifically in brain areas affected by depression.
No single mechanism explains all of exercise’s benefits on mental health. Likely they work together synergistically to bolster brain structure and function and protect it from a downward slide into mental illness.
What kinds of exercise work best?
Aerobic exercise is good.
Literally hundreds of studies have shown that aerobic activity – exercise that raises heart rate, like jogging, cycling, cross-country skiing – relieves depressive symptoms.16
Some studies show that the higher the intensity of aerobic exercise (i.e. the closer one’s heart rate reaches a maximum level), the more beneficial it is.
But…two caveats here.
First, those with heart issues or other medical conditions need to be careful with high intensity exercise. Check with your doctor before doing this.
Second, for someone struggling with depression or anxiety, embarking on a regular exercise program can be challenging enough. It becomes even more so if the exercise is too intense. This can cause depressed or anxious patients to drop out before getting any benefits.
So it’s best to start slow and work your way up gradually to a higher intensity.
Experienced exercisers may want to try high intensity interval training (HIIT), a type of exercise that alternates short bursts of very intense exercise (e.g. sprinting) with intervals of lower intensity exercise (walking or jogging). HIIT has been shown to blunt one’s reactivity to stress17 and improves symptoms of depression and anxiety in clinical populations.18
Strength training is also good.
Several studies have shown that working with weights is also good for depression and anxiety. In one study, participants who did upper and lower-body strength training exercises three times a week (3 sets of 8 repetitions) had significantly reduced depression symptoms after 10 weeks compared to a control group.19
How much and How Long?
Contributors to The Exercise Effect on Mental Health endorse the current recommendations of the American College of Sports Medicine (ACSM)20 and American Heart Association;21 that is, a combination of aerobic and strength training on all or most days of the week.
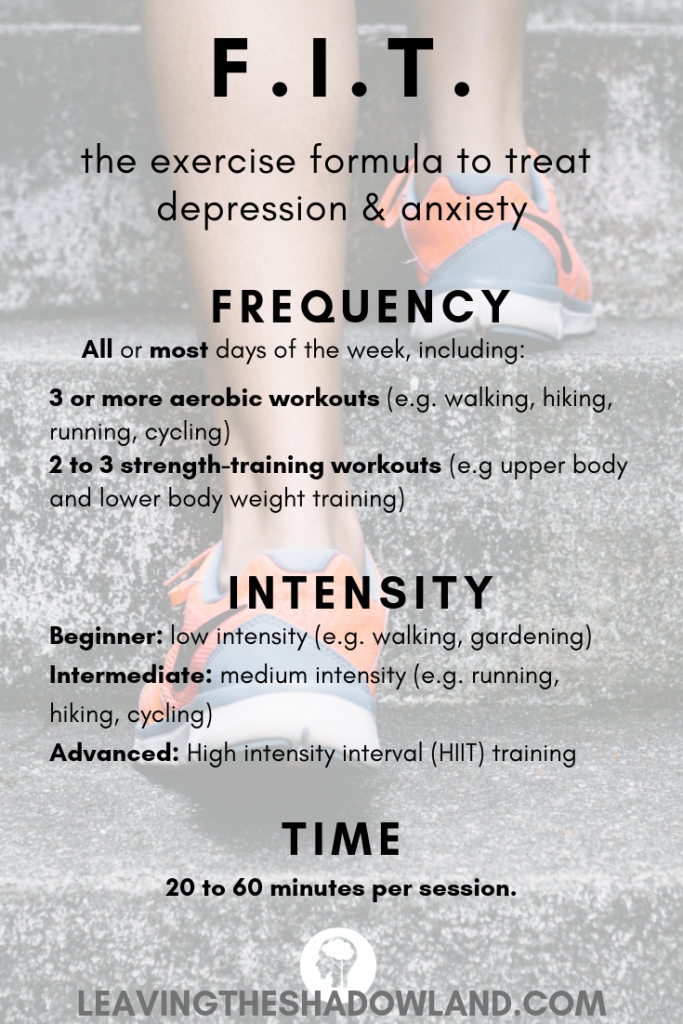
We can break that down into a F.I.T. formula that includes recommendations for frequency, intensity, and time (duration) of exercise:
- Frequency: The ACSM recommends exercising on all or most days of the week;
- Intensity: The ACSM recommends moderate to high intensity for maximum health benefits. As mentioned earlier, though, this should be weighed against the individual’s current mental state, ability to exercise, and level of physical fitness. It might be best to start with lower intensity exercise and work one’s way up to higher levels.
- Time (Duration): The ACSM recommends that each exercise session should last 20 to 60 minutes. Most mental health research indicates that you and I will need to stick to a regular exercise program for at least 8 weeks to start getting results.
Exercise should not, however, be considered a temporary fix for a specific physical or mental health challenge. Quoting the book authors: “[Exercise] should be viewed as a lifestyle modification and practiced daily throughout life.”22
Other Considerations
In order to be sustainable, exercise must be enjoyable. The United Kingdom’s Royal College of Psychiatrists gives the following advice:23
Physical Activity should:
- be enjoyable.
- help you and I to feel more competent or capable. Good examples include gardening or DIY projects.
- give a sense of control over life. It will not be helpful to view exercise as a chore that we are forced to do every day. Rather, it is something you and I choose to do in order to protect our health.
- provide a sense of escape from the stresses of life.
- be shared if possible. The companionship involved may be an important aspect of exercise’s healing benefits.
Action Steps
I hope this blog post has given you an actionable plan to start an exercise program. Start slow if you need to, but get started.
If this post has been helpful, please share it with others.
Thank you!
1 Mutrie, N., Richards, K., Lawrie, S., & Mead, G. (2018). Can Physical Activity Prevent or Treat Clinical Depression? The Exercise Effect on Mental Health: Neurobiological Mechanisms. CRC Press. pp. 380-407.
2 Scott, K. M., Lim, C., Al-Hamzawi, A., Alonso, J., Bruffaerts, R., Caldas-de-Almeida, J. M., … & Kawakami, N. (2016). Association of mental disorders with subsequent chronic physical conditions: world mental health surveys from 17 countries. JAMA psychiatry, 73(2), 150-158.
3 Chekroud, S. R., Gueorguieva, R., Zheutlin, A. B., Paulus, M., Krumholz, H. M., Krystal, J. H., & Chekroud, A. M. (2018). Association between physical exercise and mental health in 1· 2 million individuals in the USA between 2011 and 2015: a cross-sectional study. The Lancet Psychiatry, 5(9), 739-746.
4 Mammen, G., & Faulkner, G. (2013). Physical activity and the prevention of depression: a systematic review of prospective studies. American journal of preventive medicine, 45(5), 649-657.
Rebar, A. L., Stanton, R., Geard, D., Short, C., Duncan, M. J., & Vandelanotte, C. (2015). A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health psychology review, 9(3), 366-378.
5 Jonsdottir, I. H., Rödjer, L., Hadzibajramovic, E., Börjesson, M., & Ahlborg Jr, G. (2010). A prospective study of leisure-time physical activity and mental health in Swedish health care workers and social insurance officers. Preventive medicine, 51(5), 373-377.
6 McHugh, R. K., Whitton, S. W., Peckham, A. D., Welge, J. A., & Otto, M. W. (2013). Patient Preference for Psychological vs. Pharmacological Treatment of Psychiatric Disorders: A Meta-Analytic Review. The Journal of Clinical Psychiatry, 74(6), 595–602.
7 Olfson, M., & Marcus, S. C. (2010). National trends in outpatient psychotherapy. American Journal of Psychiatry, 167(12), 1456-1463.
8 Cooney, G. M., Dwan, K., Greig, C. A., Lawlor, D. A., Rimer, J., Waugh, F. R., … & Mead, G. E. (2013). Exercise for depression. Cochrane database of systematic reviews, (9).
9 Wipfli, B. M., Rethorst, C. D., & Landers, D. M. (2008). The anxiolytic effects of exercise: a meta-analysis of randomized trials and dose–response analysis. Journal of Sport and Exercise Psychology, 30(4), 392-410.
10 Mutrie, N., Biddle, S. J. H., & Gorely, T. (2015). Psychology of physical activity. Florence: Taylor and Francis.
11 Boecker, H., Sprenger, T., Spilker, M. E., Henriksen, G., Koppenhoefer, M., Wagner, K. J., … & Tolle, T. R. (2008). The runner’s high: opioidergic mechanisms in the human brain. Cerebral Cortex, 18(11), 2523-2531.
12 Wegner, M., Helmich, I., Machado, S., E Nardi, A., Arias-Carrión, O., & Budde, H. (2014). Effects of exercise on anxiety and depression disorders: review of meta-analyses and neurobiological mechanisms. CNS & Neurological Disorders-Drug Targets (Formerly Current Drug Targets-CNS & Neurological Disorders), 13(6), 1002-1014.
13 Rethorst, C. D., Toups, M. S., Greer, T. L., Nakonezny, P. A., Carmody, T. J., Grannemann, B. D., … & Trivedi, M. H. (2013). Pro-inflammatory cytokines as predictors of antidepressant effects of exercise in major depressive disorder. Molecular psychiatry, 18(10), 1119.
14 Burdette, J. H., Laurienti, P. J., Espeland, M. A., Morgan, A. R., Telesford, Q., Vechlekar, C. D., … & Rejeski, W. J. (2010). Using network science to evaluate exercise-associated brain changes in older adults. Frontiers in aging neuroscience, 2, 23.
15 Voss, M. W., Vivar, C., Kramer, A. F., & van Praag, H. (2013). Bridging animal and human models of exercise-induced brain plasticity. Trends in cognitive sciences, 17(10), 525-544.
16 Alderman, B. L., & Olson, R. L. (2018). Prescribing Exercise for Mental Health. The Exercise Effect on Mental Health: Neurobiological Mechanisms. CRC Press. pp. 411-441.
17 Lark, S., Kurtovich, R., de Terte, I., & Bromhead, C. (2018). The Effect of High-Intensity Intermittent Exercise on Chronic Stress and Potential Biomarkers: a Pilot Study. Journal of Police and Criminal Psychology, 1-8.
18 Freyssin, C., Verkindt, C., Prieur, F., Benaich, P., Maunier, S., & Blanc, P. (2012). Cardiac rehabilitation in chronic heart failure: effect of an 8-week, high-intensity interval training versus continuous training. Archives of physical medicine and rehabilitation, 93(8), 1359-1364.
19 Singh, N. A., Clements, K. M., & Fiatarone, M. A. (1997). A randomized controlled trial of progressive resistance training in depressed elders. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 52(1), M27-M35.
20 American College of Sports Medicine. (2013). ACSM’s guidelines for exercise testing and prescription. Lippincott Williams & Wilkins.
21 Haskell, W. L., Lee, I. M., Pate, R. R., Powell, K. E., Blair, S. N., Franklin, B. A., … & Bauman, A. (2007). ACSM/AHA Recommendations. Circulation, 116(9), 1081-1093.
22 Alderman, B. L., & Olson, R. L. (2018). Prescribing Exercise for Mental Health. The Exercise Effect on Mental Health: Neurobiological Mechanisms. CRC Press. p.435.
23 Mutrie, N., Richards, K., Lawrie, S., & Mead, G. (2018). Can Physical Activity Prevent or Treat Clinical Depression? The Exercise Effect on Mental Health: Neurobiological Mechanisms. CRC Press. p.401.

Dr. Pamela Coburn-Litvak has published research articles on exercise and stress in Neuroscience and Neurobiology of Learning and Behavior. Her latest book, Leaving the Shadowland of Stress, Anxiety, and Depression, was published in 2020.
After receiving a Ph.D. in Neurobiology and Behavior from the State University of New York at Stony Brook, she served as both Assistant Professor of Physiology & Pharmacology and Special Assistant to the Vice President for Research Affairs at Loma Linda University in Loma Linda, California. She then joined the Biology department at Andrews University and developed courses in human physiology as well as the neurobiology of mental illness. She also founded Rock @ Science LLC, a company that specializes in health and science education and web development. She co-developed the brain and body physiology segment of the Stress: Beyond Coping seminar with its creator, Dr. William “Skip” MacCarty, DMin.
Dr. Coburn-Litvak currently lives in California with her husband. Their two daughters are mostly grown and attending school elsewhere.
When she’s not studying or teaching about stress, she enjoys stress-relieving activities like puttering around the garden, taking nature walks with her family, knitting, cooking, and reading.
