
We feel the way we think.
This is a 6-word summary of a type of psychotherapy called Cognitive Behavioral Therapy, CBT for short.
CBT was first developed in the 1950s and 60s by psychiatrist Aaron T. Beck (and others including clinical psychologist Albert Ellis). At that time, psychoanalysis was still all the rage – this is the type of psychotherapy often depicted with a patient laying on the couch, spilling his or her mental guts to a therapist in hopes of making logical connections between conscious problems and unconscious causes (e.g. repressed fears or conflicts).
Carefully designed research studies were conducted to evaluate psychoanalytic methods for treating mental disorders like depression. Dr. Beck expected his methods to pass with flying colors, but they didn’t. He was shocked to find just the opposite – the research failed to validate psychoanalysis as a tool for treating depression.1
Which left Dr. Beck wondering what methods would work. He and his colleagues developed a new form of psychotherapy, based on three principles:
Cognitive Behavioral Therapy Principle #1: The way we think about things determines how we feel about them.
An illustration might be helpful here. We often think that this is how we get into a bad mood:
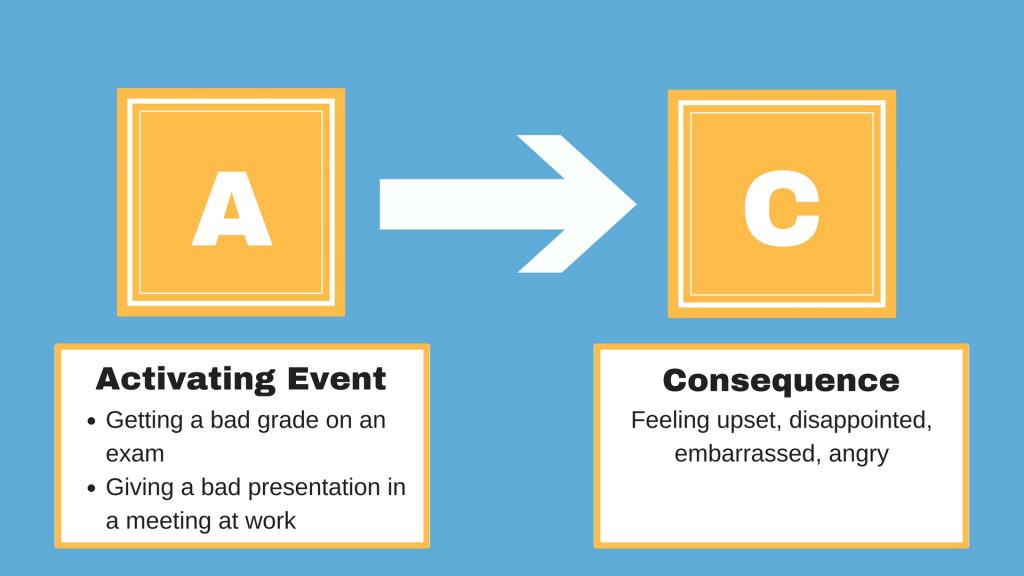
When we work really hard at something, we commonly feel disappointed and upset when we don’t do as well as we wanted to.
But think about that last sentence for a minute – the reason why we are upset is not really the presentation or test results, but an unfulfilled expectation or hope that we had for them.
In other words, the Activating event (A) does NOT lead directly to the Consequence (C). There is something else inserted in the middle:
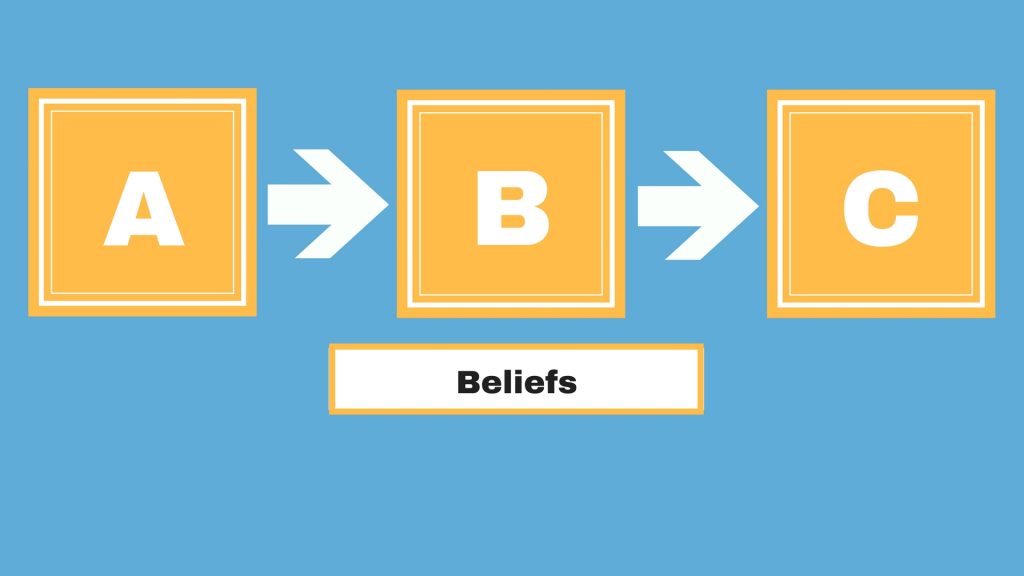
The first principle of CBT is that everything that happens to us is mentally filtered through our Beliefs (B).
Well, the technical term is “Cognitions,” which casts a wider net – cognitions include our beliefs, perceptions, attitudes, expectations, and mental interpretations of what is going on around us.
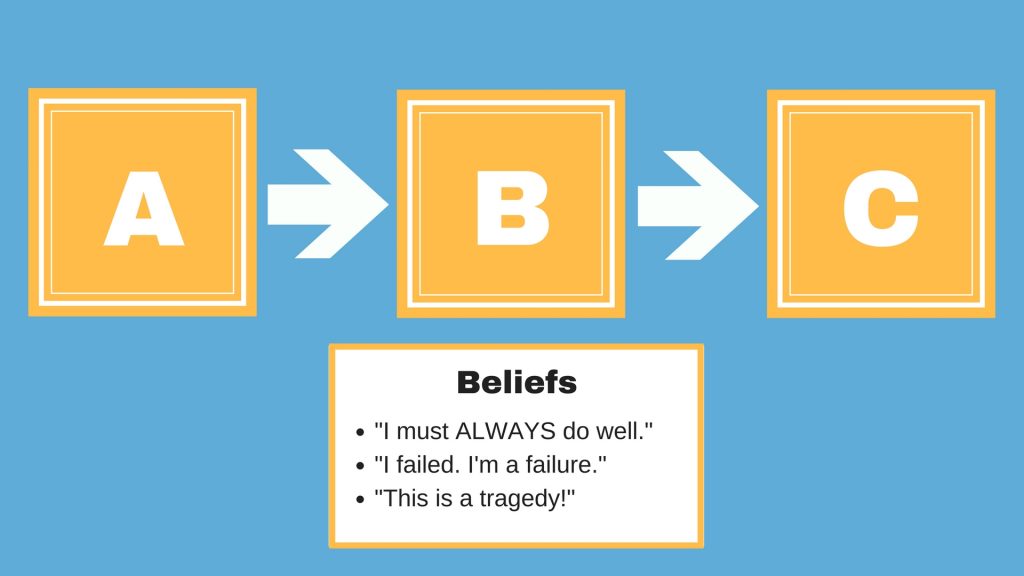
There could be several cognitions that contribute in this case:
Dr. Beck and his colleagues did not invent this idea – various philosophers have been spouting it for over 2500 years.
It is also a pervasive concept in current psychology textbooks. In the textbook Stress and Health: Biological and Psychological Interactions, biological psychologist William Lovallo wrote the following:
We may find that a major personal disappointment, say failing to get into graduate school, causes great emotional distress. Or the sound of footsteps on a dark street may provoke a feeling of terror. The disappointment may evoke physical sensations of sadness, lethargy, or even tears of grief. The footsteps may result in fear along with a racing heart and rapid breathing. The key point to these two examples is that the individual’s physiological responses started out as thoughts and interpretations, mental events that are not in fact physically threatening, and which in a real sense are not things at all. The emotions and physiological responses arose because of his or her interpretation of the event and its perceived meaning in terms of his or her well-being (italics mine).”2
Dr. Beck’s novel contribution was to apply this principle to the psychotherapeutic treatment of depression in ways that had never been thought of before. And then, he and his colleagues added two more principles:
Cognitive Behavioral Therapy Principle #2: Depression is dominated by negative beliefs or cognitions.
We who have suffered or are suffering from depression know what this means. We have felt the effects of it, even if we have never articulated it in this way before.
Depression means that we see the world as a shadowland, a dark, desolate place filled with danger and despair.
Severe depression may cause us to believe that the world has always been that way and will continue to be that way forever. It is this grim vision of the future that creates one of depression’s most debilitating symptoms: hopelessness.
But in many cases, it is our beliefs and perceptions that cast the shadows, not our circumstances themselves.
I can already hear some of you disagreeing with me. “What do you mean, it’s just our perceptions and beliefs? Are you saying that nothing bad ever happens in the world that should sadden, disappoint, or sometimes scare the pants off of us?”
No, I’m not saying that the world is a perfect place where nothing bad ever happens, or that the sun is always shining while we, the depressed, cry under our imaginary raincloud.
But let’s agree that reality lies somewhere in between a shadowland and a land of eternal sunshine.
Bad things do happen, and it is okay to feel upset or grieved over those things. But depression mentally skews our view of the world toward the shadows. And this leads us to the third principle of CBT.
Cognitive Behavioral Therapy Principle #3: In Depression, negative emotions are nearly always generated by cognitive distortions.
My earlier point probably bears repeating: it is natural and right to feel upset when bad things happen. In fact, I’ll say it in an even stronger way: our negative emotions (e.g. fear or sadness) actually serve a vital purpose: they are our mind’s alert signals to let us know when something is indeed wrong or dangerous.
Disappointment over a poor grade is a minor example, but still illustrates the point: if we don’t feel disappointed, we are not motivated to do better in the future. Or take one of Dr. Lovallo’s examples: if we don’t have a healthy fear of dark alleys, we will nonchalantly wander into several until we meet an untimely end.
So the problem is not with the emotions themselves.
Rather, the problem in depression is almost always the underlying belief that causes the emotion. These beliefs are almost always distorted to give us a twisted and unrealistic view of the world.
While it is natural and healthy to feel disappointment over a poor grade or poor work performance (in the sense that it will spur you on to do better next time), it is unnatural and unhealthy to emotionally fall apart over these things.
Such emotional meltdowns are almost always due to an unhealthy perception, belief, attitude, or expectation you had about that event.
Here is an example: “I got a C on that test — that means I am a complete failure and I will never graduate and I will never get a job and I will never be able to support my family and my spouse and kids will eventually leave me and I will grow old and die alone and miserable.” Such strings of cognitive distortions can easily turn a minor disappointment into a major emotional crisis.
It’s like looking into a funhouse mirror.

It is, in one sense, still an image of you – it is made of the same light rays that bounce off your body onto a regular mirror and back onto your retina.
But of course, in the real sense, it is not the way you look at all. The distortions of the mirror’s surface cause the light rays to bounce and bend in ways that distort the image.
Cognitive distortions are the funhouse mirrors of the mind. They bounce and bend incoming information in ways that distort our mental image of reality.
Here’s the key point: distorted cognitions are bound to cause distorted emotions. This is how we skew our world to the negative, making us see danger and disappointment that is actually not there.
The goal of CBT is to pinpoint and eliminate the cognitive distortions in order to eliminate the distorted emotions.
So the next step is to describe the main types of cognitive distortions. And that is what we will do in the rest of this 101 series.3
Conclusion and Action Steps
- Keep a thought journal for the next few days. Take note of the times during the day when you feel frustrated, angry, or sad about something that happened. Write down your thoughts about that event. Don’t judge your thoughts at this point; just write them down.
- In order to identify possible distortions in your thoughts, continue reading this 101 series.
1 https://beckinstitute.org/about-beck/our-history/history-of-cognitive-therapy/
2 Lovallo, W. R. (2015). Stress and health: Biological and psychological interactions. Sage publications.
3 I am indebted to Dr. David Burns, a colleague of Aaron Beck, who wrote the classic book Feeling Good: The New Mood Therapy. Most of what I have written here is adapted from Chapter 1.
Burns, D. D. (1981). Feeling good. Signet Book. pp.9-13.

Dr. Pamela Coburn-Litvak has published research articles on exercise and stress in Neuroscience and Neurobiology of Learning and Behavior. Her latest book, Leaving the Shadowland of Stress, Anxiety, and Depression, was published in 2020.
After receiving a Ph.D. in Neurobiology and Behavior from the State University of New York at Stony Brook, she served as both Assistant Professor of Physiology & Pharmacology and Special Assistant to the Vice President for Research Affairs at Loma Linda University in Loma Linda, California. She then joined the Biology department at Andrews University and developed courses in human physiology as well as the neurobiology of mental illness. She also founded Rock @ Science LLC, a company that specializes in health and science education and web development. She co-developed the brain and body physiology segment of the Stress: Beyond Coping seminar with its creator, Dr. William “Skip” MacCarty, DMin.
Dr. Coburn-Litvak currently lives in California with her husband. Their two daughters are mostly grown and attending school elsewhere.
When she’s not studying or teaching about stress, she enjoys stress-relieving activities like puttering around the garden, taking nature walks with her family, knitting, cooking, and reading.

[…] is the most extensively studied among several psychotherapy methods used for these disorders. In Part 1, I explained that psychiatrist Aaron T. Beck and his colleagues developed CBT because […]
[…] Read the next part of this 101 series. Or you can read the previous part. Or you can start from the beginning. […]
[…] Read the next part of this 101 series. Or you can start at the beginning here. […]
[…] Read the next part of this 101 series. Or you can read the previous part. Or you can start from the beginning. […]
[…] Read the next part of this 101 series. Or you can read the previous part. Or you can start from the beginning. […]
[…] Read the next part of this 101 series. Or you can read the previous part. Or you can start from the beginning. […]
[…] discussed positive self-talk at length in my Cognitive Behavioral Therapy 101 series. When something bad happens, it is natural to ask ourselves why. To put thinking patterns in […]
[…] my previous series on Cognitive Behavioral Therapy, I talked about negative mental filters: thinking patterns that filter out the good aspects of any […]
[…] year in my blog, I wrote a long series on cognitive behavioral therapy, including the distorted beliefs we sometimes use. What would happen if, instead of using distorted […]
[…] In previous posts, I have addressed ways to restore brain imbalance through a popular form of therapy called Cognitive Behavioral Therapy. […]
[…] very powerful form of therapy called Cognitive Behavioral Therapy, CBT for short. I’ve done a series on CBT before, but it’s a topic worth covering […]
[…] of you may be familiar with my earlier series on cognitive behavioral therapy. I’m re-visiting these concepts as a follow-up to my more recent series on the Four Roads out […]