
This website is all about exploring the relationship between stress and two of the most common mental disorders in the world today: depression and anxiety.1
Clinical depression affects about 62 million individuals in the United States alone and about 300 million worldwide.2
Clinical anxiety (e.g. generalized anxiety disorder, social anxiety, panic disorder, etc.) makes us feel anxious and fearful, even when there’s nothing to be afraid of.
The World Health Organization estimates that about 260 million people around the world suffer from an anxiety disorder.3
We might be tempted to think then that, between the two mind-brain disorders, 600 million people are affected. But this would be wrong, because often these disorders go hand-in-hand in the same individuals.
Imagine what that would be like. Imagine constantly living with a choking sense of fear, while your heart is weighted down with despair.
If you’ve never felt the crippling weight of both together (and I have), it’s almost impossible to describe.
Sadly, the overlap between depression and anxiety is pretty high – somewhere between half and three quarters of individuals who have one will also struggle with the other.
The question is, why?
Why do these debilitating disorders so often go together?
In this blog post, I will explain exactly how this happens. To do this, I’m going to dig into some neuroscience, showing how different parts of the brain work together and what happens when they malfunction.
I have some very important reasons for doing this.
First, I truly believe that knowledge is power. When we understand what lies behind our depression and anxiety, we stand a much better chance of beating them.
Second, understanding some basic brain science helps to point us to the best treatments for these disorders. And given the high overlap, ideally we would want to use treatments that work equally well for both depression and anxiety.
It’s helpful then to know a little bit about how and why these mind-brain disorders develop together in the brain.
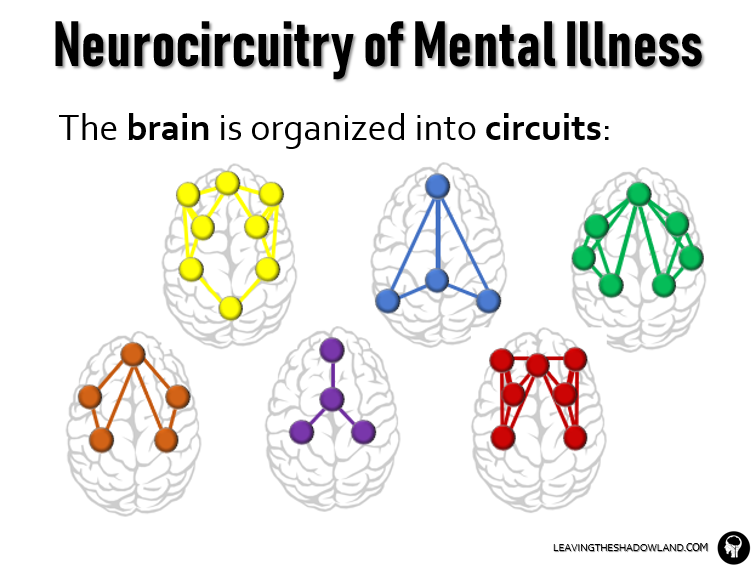
The brain is organized into circuits.
Before we start, I just want to give a shout-out to psychiatrist Leanne Williams at Stanford University, an amazing scientist whom I love.
Yes, even the world of neuroscience has its rock stars – Dr. Williams is definitely one for me.
Much of the information in this post is taken from her research.4
The brain is an information superhighway, with literally trillions of messages being sent and received all the time.
In order to best organize this information, the brain is organized into multiple circuits – groups of brain areas that process specific types of information.
Just like the electronic circuits in your laptop or smartphone, each brain circuit can have a range of activity levels. Ideally, they work at a normal level, but with different pathologies they may work more sluggishly than normal (“under-active”) or conversely at a higher, fever-pitch (“over-active”).
We think that different combinations of abnormal activity is what causes different mind-brain disorders. The symptoms of the disorder would reflect the abnormal activity in the brain circuits.
We use a lot of different circuits in our daily lives.
Example Scenario: Think about what you are doing as you drive your car down the road. In addition to driving, you are probably also planning your day or thinking about what happened that day.
The Brain “at rest”
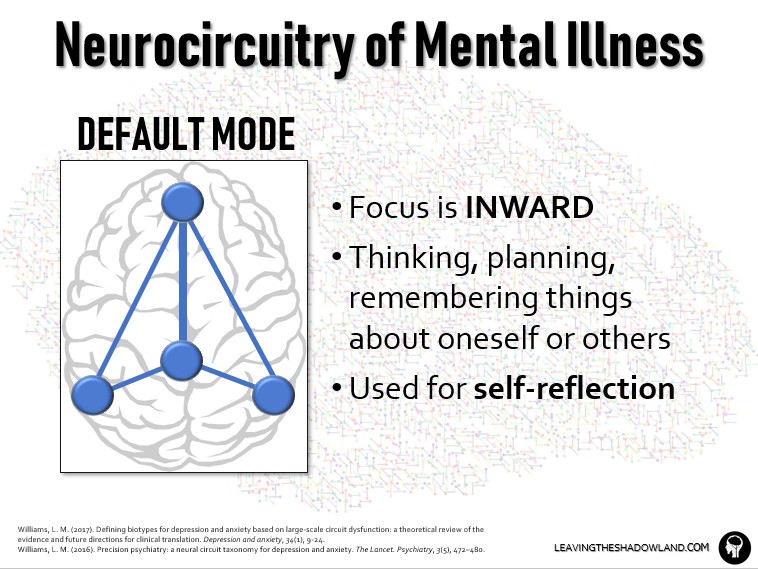
The Default Circuit is a group of brain structures that are active when the brain is “at rest.”
In other words, these structures are turned on “by default” when we are not engaged with the external world, but instead are engrossed in our internal world. So the focus is INWARD.
This brain circuit is active during daydreaming and mind-wandering, reflecting on oneself or others, reminiscing about the past, or planning for the future.
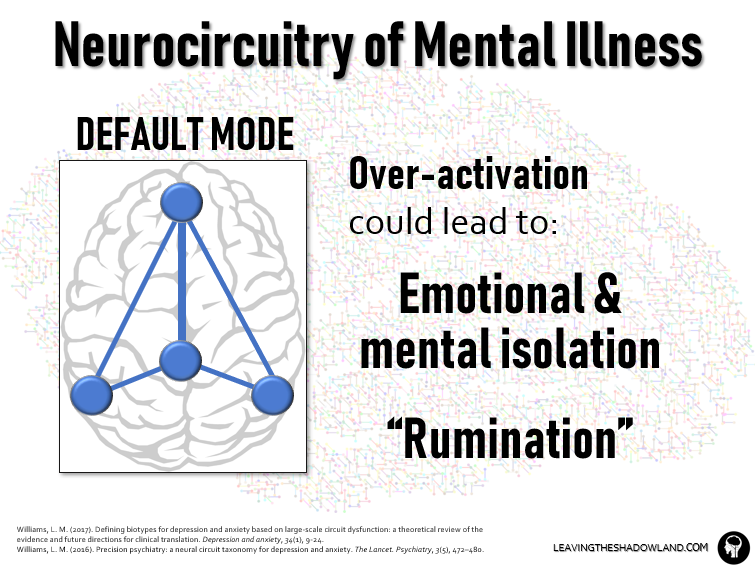
It stands to reason that OVERACTIVATION in this circuit could lead to emotional and mental isolation, becoming a mental recluse, causing one to live exclusively in the internal world.
This overactivation twists the mind constantly inward, into a deep place filled with dark thoughts. These thoughts are endlessly, obsessively replayed in the individual’s mind in a process called “rumination.”
High levels of rumination predict the onset of depression in the non-depressed individuals and more severe symptoms in the depressed.
Brain Switch for “Salience”
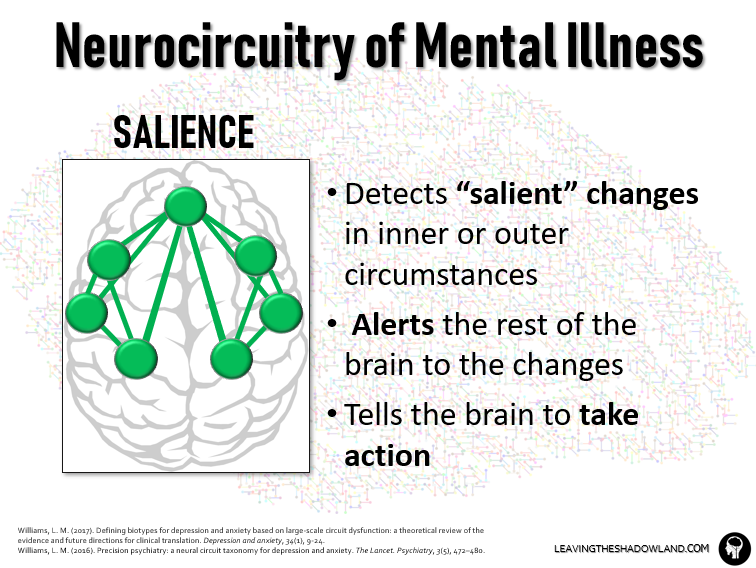
We are constantly bombarded with information about both the outside world and our internal state of mind.
Normally, 99% of the information is scanned briefly and then ignored.
The brain is adept at sifting through and identifying the most “salient” information that may most significantly impact us or threaten our well-being.
The Salience Circuit is a cluster of brain areas responsible for detecting salient changes in inner or outer conditions and then telling other brain circuits to take action.
Example Scenario: As you are driving down the road, a car suddenly swerves into your lane right in front of you. The salience circuit tells you to pay attention to this important or salient information.
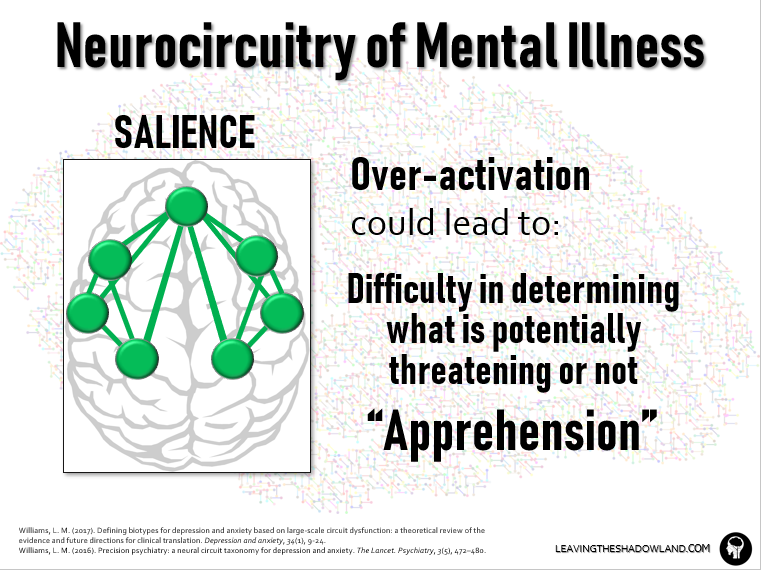
It stands to reason that OVERACTIVATION of this circuit could lower the brain’s threshold for determining salience, making it difficult to distinguish between what is potentially threatening and what is not.
This can lead to the symptom of APPREHENSION, being on high alert all the time, waiting for something to happen. This, of course, is a very common symptom of anxiety disorders, but can also occur in depression.
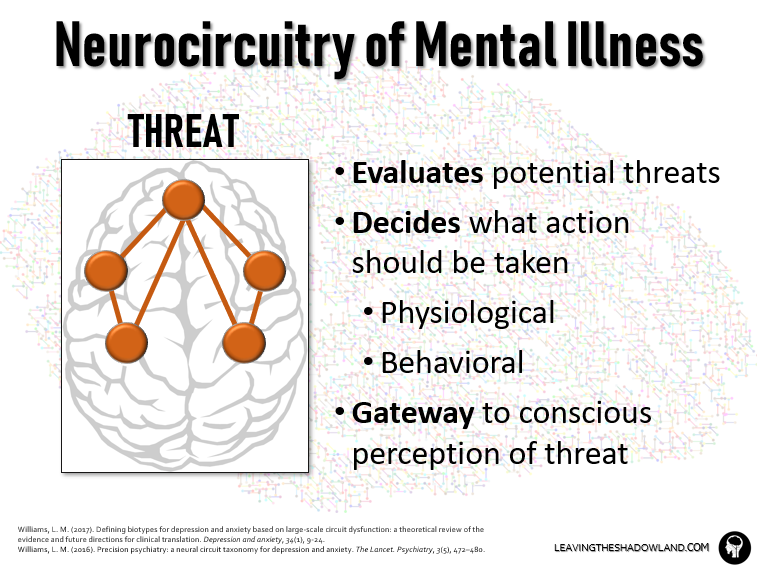
The Brain Response to Threat
Like all of God’s creatures, we humans must pay attention to and react to potential threats in our environment.
The threat circuit is a cluster of brain structures that evaluates potential threats. If you see some overlap between this circuit and the salience circuit, you’re right — some brain structures are a part of both. But they have distinct functions: the salience circuit first alerts us to a potential threat; the threat circuit decides just how threatening the threat is and decides what action should be taken.
Example Scenario: After the car swerves into your lane, the threat circuit decides what action should be taken. It triggers the stress response, emotional responses (fear), and behavioral responses.
Here’s another interesting note about the threat circuit: it can operate below the level of conscious awareness.
We know this through several brain imaging studies in which subjects were shown pictures of threatening facial expressions. However, the images were “masked” in some cases: an angry or fearful face was displayed for only a few milliseconds, not long enough to trigger conscious perception, then “masked” by a longer display of a neutral face. Brain regions in the threat circuit were activated regardless of this masking. The threat circuit does eventually send the information to higher levels of brain, the cerebral cortex — this is when we become consciously aware of our fear and anxiety.
In humans, the threat circuit is commonly activated by others’ facial expressions that may mean imminent danger: anger, disgust, contempt, guilt, fear, or nervousness. One part of the circuit evaluates the threat (e.g. my boss’s angry face) and makes a plan to adapt to or avoid it: make a groveling apology for my latest report, or alternatively stand my ground to defend it. Or call in sick the next day. Another part of the circuit regulates our emotional reaction to the threat (e.g. fear, anxiety, defensiveness) and tries to ease this reaction when appropriate.
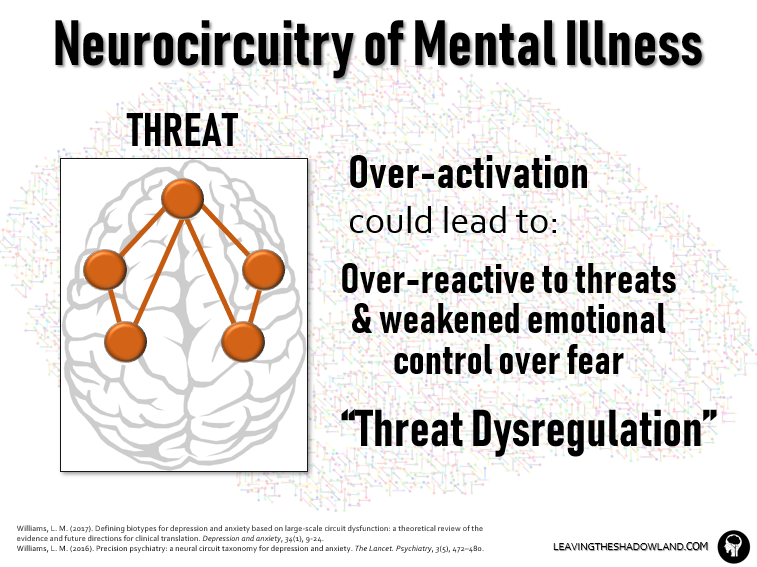
Logically, OVER-ACTIVATION in the first part could make us overly-reactive to threat, while UNDER-ACTIVATION in the second part could weaken control over our feelings about threat.
Together, these both contribute to an anxiety symptom called “threat dysregulation.”
Paying Attention
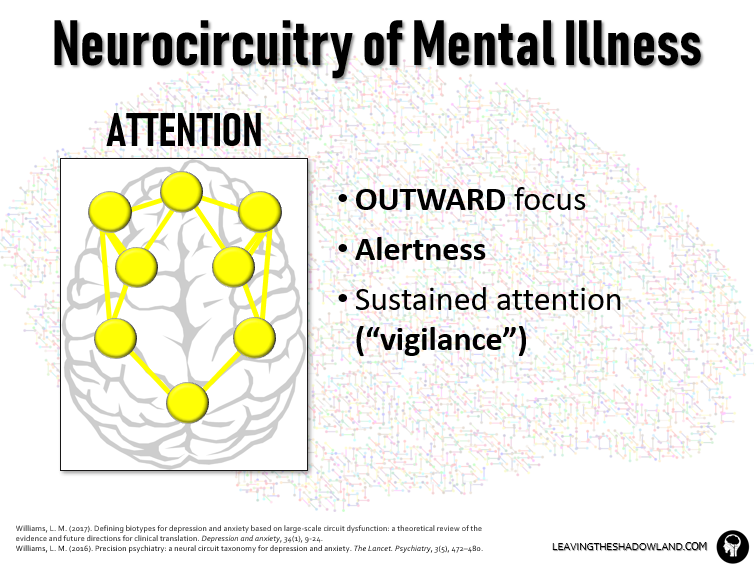
The Attention Circuit is kind of the flip side of the Default Circuit.
It in fact interacts with the Default Circuit in order to shift the brain from a reflective resting state to one that is alert, outwardly focused, and activated in task-specific ways.
This circuit creates alertness, helping us focus on the task at hand. It also supports recall of information.
It also works with the threat circuit to create a state of sustained attention in potentially threatening environments: vigilance.
Example Scenario: The attention circuit is what helped you focus on other cars on the road on the rest of your drive.
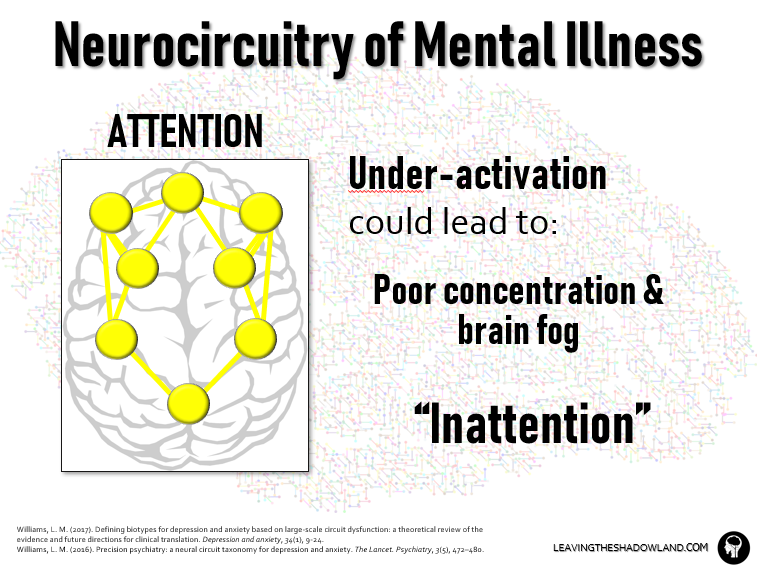
It stands to reason, then, that UNDER-ACTIVATION and connectivity in this circuit could produce a sustained state of brain fog, an inability to concentrate or even remain alert to the outside world.
Depressed individuals often suffer from this kind of “inattention.”
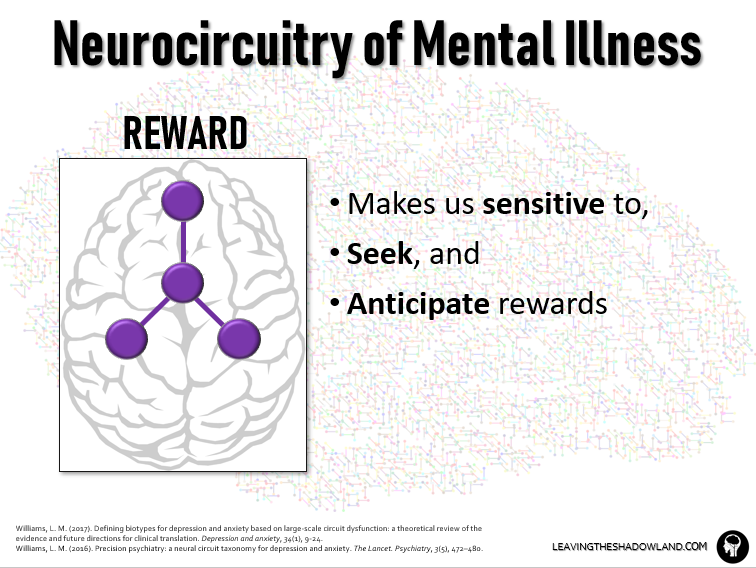
Seeking Reward
Example Scenario: After the car swerves into your lane and you successfully avoid a crash, you say to yourself, “I deserve something sweet to reward myself for driving so carefully.” So you stop by the ice cream shop on the way home.
The Reward Circuit makes us sensitive to, seek, and anticipate rewarding stuff in our lives: pleasant tastes or sights or sounds, fulfilling hobbies or pursuits, good vibes in relationships.
An appreciation of these things will encourage us to seek out more of the same in the future.
Brain regions in this circuit release the neurotransmitter dopamine, which regulates our motivation and desire for rewarding stimuli and may also help create subjective feelings of pleasure.
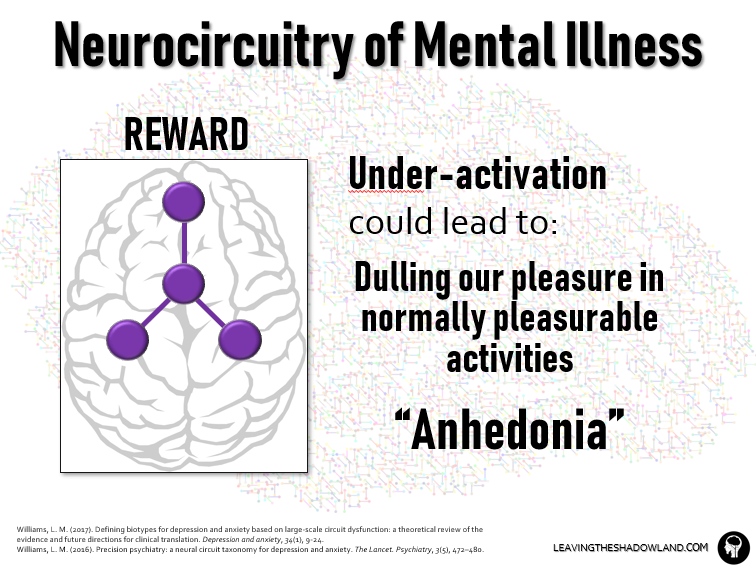
Logically, UNDER-ACTIVATION in this circuit can take the shine off of previously enjoyable activities and dull our pleasure in them. Chocolate may taste less sweet; our past recollections of enjoying it would fade, and we would be less likely to go out and buy more. (How tragic.)
The same would hold true for any rewarding activity or relationship.
This “dulled pleasure” in life is a common symptom of depression called “Anhedonia.”
The Brain’s CEO
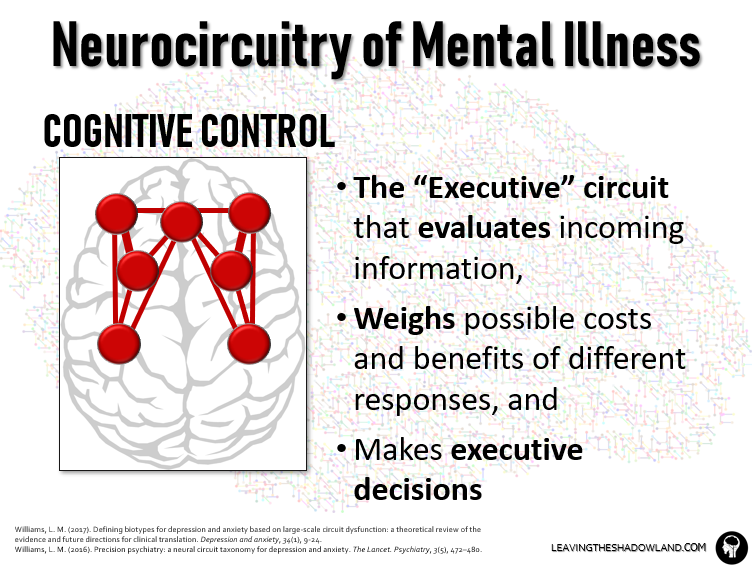
The Cognitive Control Circuit is also called the Executive Circuit because it has executive status among all brain circuits.
It includes the highest ranking regions in the brain in terms of the information they receive and the authoritative power they wield over the other circuits.
Working at this high level requires the ability to focus on pertinent information and weigh the possible costs (threat) and benefits (reward) of different responses.
The cognitive control circuit assembles the right team to accomplish these complex tasks: structures for attention and working memory, flexible decision-making, and suppression of unhelpful responses.
Example Scenario: Your cognitive control circuit helps you make the wise choice to forgo the ice cream and leave the ice cream store.
How Brain Circuits Work Together
A healthy brain runs like a well-organized and efficient company.
Executive leadership at the top makes well-informed, competent decisions to regulate the actions of multiple departments. The departments (brain circuits) in turn are allowed to function independently, but not in isolation, from each other.
Cross-communication is facilitated by certain brain areas acting as common “hubs” for multiple brain circuits. Neural signals can pass through one circuit and then move on to another through one or more of these communication hubs.
Healthy brain functioning thus requires, not just the healthy functioning of each circuit, but a balance in communication and power between circuits.
Glitches in one or more of these areas will send unsettling shock waves through the whole organization.
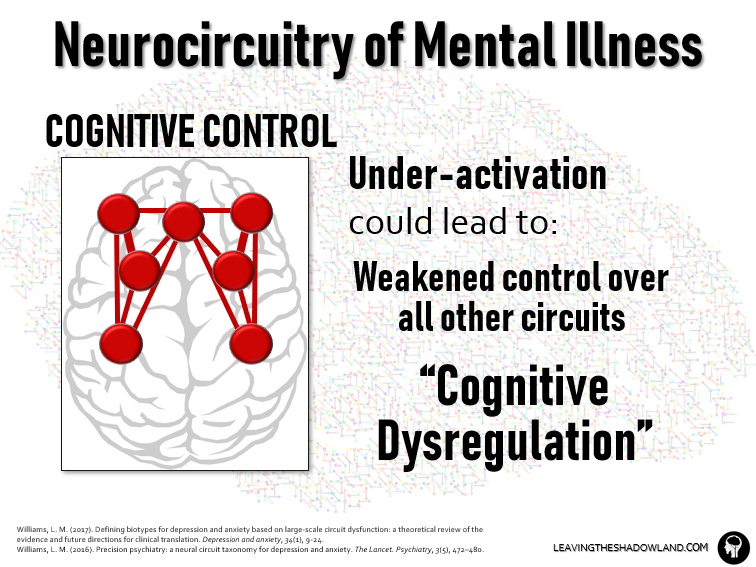
It logically follows that dysfunction in the brain’s executive leadership could have the most devastating and pervasive impact of all.
UNDER-ACTIVATION of this circuit weakens its authority and undermines communication with other brain circuits. This is called “cognitive dysregulation.”
What Happens in Depression and Anxiety
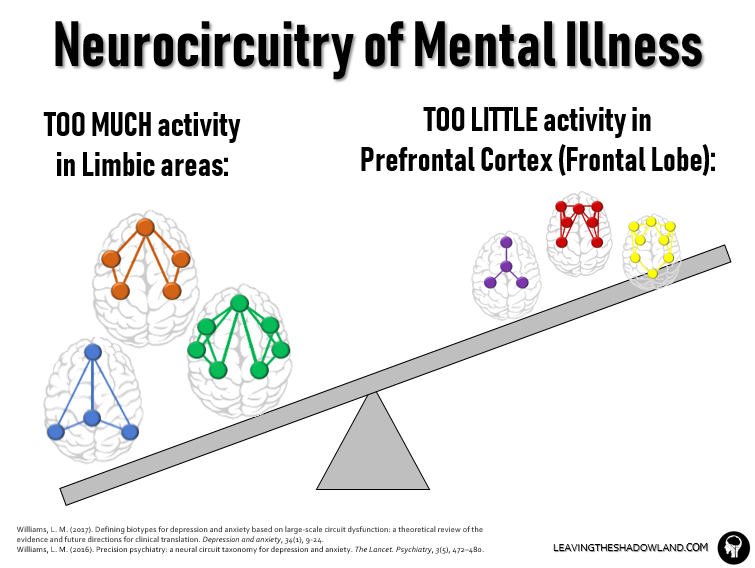
In broad terms (and I’m simplifying a bit here), what we see with the mind-brain disorders of depression and anxiety is too much activity in the “feeling” areas of the brain (anterior insula, amygdala) and too little activity in the “thinking” areas (frontal lobe, especially the prefrontal cortex).
This is not to say that emotion is all bad and analytical thinking is everything good. Just that, in mental disorders, they are out of proper balance.
Three Take-Aways
Thanks for sticking with me through that journey through the brain. Here are three important take-aways:
#1. Depression and anxiety disorders are real.
This should really go without saying, but unfortunately, some still believe that depression and anxiety are not real, that people just make them up to get attention.
But we neuroscientists know for a fact that they are real, in the sense that we can measure them with scientific instruments. We can measure differences in brain activity between healthy patients and those with these disorders. We can also see differences in physical size, or in brain cell numbers. This should help to combat the stigma that we seem to have toward these disorders.
#2. Depression and Anxiety SHARE many of the same patterns of abnormal brain activity.
This answers the main question of this post and helps to explain the 50-70% overlap between depression and anxiety. Too many of us know from personal experience that depression can be riddled with fear and anxiety, while anxiety disorders can be riddled with feelings of hopelessness and despair.
But this begs another question: If similar activity patterns are seen in both, why isn’t there 100% overlap between depression and anxiety?
One reason is, the pattern is not exactly the same. I glossed over some differences seen in the attention and salience circuits, for example.
Another reason is, the point of origin, where the damage started, can be different between disorders. With anxiety disorders that start with a trauma (e.g. PTSD), the triggering event for the disorder is usually a direct hit to the brain areas involved in the threat circuit. That’s ground zero. Then the damage spirals outward from that point to include other circuits.
In depression, the damage can be in lots of places, particularly the cognitive control circuit, default, and reward circuits.
But here is the most important point of all:
#3: Understanding these brain circuits can point us to the best treatments.
The best treatments will:
- Promote overall brain health – we want to make sure our lifestyle choices are supporting the best mental health possible;
- Repair brain damage that has occurred in specific brain circuits; and
- Restore brain imbalance, particularly in the thought patterns we use.
In previous posts, I have addressed ways to restore brain imbalance through a popular form of therapy called Cognitive Behavioral Therapy.
For the next couple months, I will be talking about specific ways to promote brain health.
Specifically, I will be talking about nutrition.
Next week, we will kick things off by comparing the best diet for mental health vs. the worst. See you then!
1 The Diagnostic and Statistical Manual of Mental Disorders, 5th edition, published by the American Psychiatric Association in 2013
2 https://www.who.int/news-room/fact-sheets/detail/depression
3 https://www.who.int/mental_health/management/depression/prevalence_global_health_estimates/en/
4 Williams, L. M. (2017). Defining biotypes for depression and anxiety based on large‐scale circuit dysfunction: a theoretical review of the evidence and future directions for clinical translation. Depression and anxiety, 34(1), 9-24.
Williams, L. M. (2016). Precision psychiatry: a neural circuit taxonomy for depression and anxiety. The Lancet. Psychiatry, 3(5), 472–480.

Dr. Pamela Coburn-Litvak has published research articles on exercise and stress in Neuroscience and Neurobiology of Learning and Behavior. Her latest book, Leaving the Shadowland of Stress, Anxiety, and Depression, was published in 2020.
After receiving a Ph.D. in Neurobiology and Behavior from the State University of New York at Stony Brook, she served as both Assistant Professor of Physiology & Pharmacology and Special Assistant to the Vice President for Research Affairs at Loma Linda University in Loma Linda, California. She then joined the Biology department at Andrews University and developed courses in human physiology as well as the neurobiology of mental illness. She also founded Rock @ Science LLC, a company that specializes in health and science education and web development. She co-developed the brain and body physiology segment of the Stress: Beyond Coping seminar with its creator, Dr. William “Skip” MacCarty, DMin.
Dr. Coburn-Litvak currently lives in California with her husband. Their two daughters are mostly grown and attending school elsewhere.
When she’s not studying or teaching about stress, she enjoys stress-relieving activities like puttering around the garden, taking nature walks with her family, knitting, cooking, and reading.

